
Investigating the effects and efficacy of self-compassion intervention on generalized anxiety disorders
Do you remember the dread of presenting in front of a crowd, or does even the thought make you uneasy? For some, anxiety is a


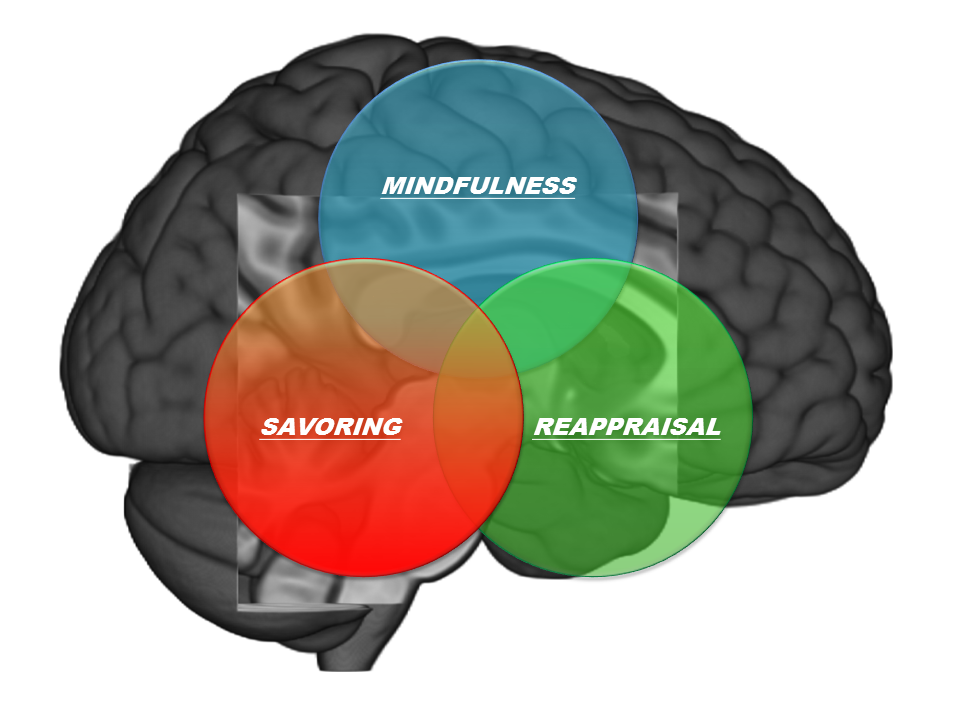
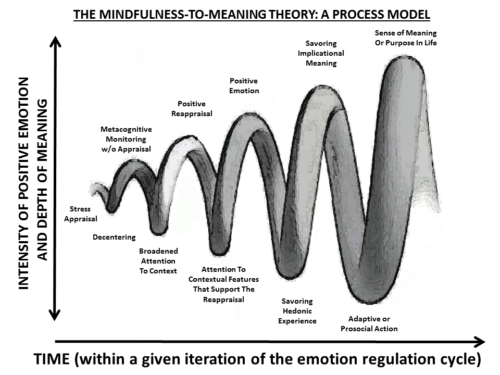
Dr. Eric Garland, PhD, LCSW is Presidential Scholar, Associate Dean for Research, and Professor in the University of Utah College of Social Work, Director of the Center on Mindfulness and Integrative Health Intervention Development (C-MIIND), and Associate Director of Integrative Medicine in Supportive Oncology and Survivorship at the Huntsman Cancer Institute. Dr. Garland is the developer of an innovative, multimodal mindfulness-based intervention founded on insights derived from cognitive, affective, and neurobiological science, called Mindfulness-Oriented Recovery Enhancement (MORE).

Do you remember the dread of presenting in front of a crowd, or does even the thought make you uneasy? For some, anxiety is a

“Self-compassion emerged as a crucial factor for mental toughness. Athletes who treated themselves with kindness and understanding were more confident, resilient, and capable of coping

“These results highlight that trauma-sensitive interventions could be combined with mindfulness and self-compassion interventions to address the unique presenting clinical problems of those who experienced

“The findings do support existing theories that link self-compassion to the ability to receive compassion from others, which is often fostered through secure attachment relationships.

This study investigates the impact of humane education on fostering empathy and compassion towards animals within the Indian adolescent population. It addresses the escalating concerns

“Fostering self-compassion and building strong support systems empowers educators and counselors to guide students through mental distress, enhancing their well-being and resilience.” This study investigated

“Even if they felt excluded, those who had greater levels of self-compassion exhibited less depression because they tended to use positive coping mechanisms. “

The study also highlighted how emotional well-being and self-compassion act as mediators, bridging the gap between mental toughness and aggression to strengthen the protective impact of mental toughness against aggression.

The research highlights the importance to encourage self-compassion and forgiveness to improve older people’s mental health

Recent studies investigating the relationship between loneliness and poor sleep quality in teenagers discovered a significant correlation between higher loneliness and poorer sleep quality.

Dr. Linda Carlson holds the Enbridge Research Chair in Psychosocial Oncology, is Full Professor in Psychosocial Oncology in the Department of Oncology, Cumming School of Medicine at the University of Calgary, and Adjunct Professor in the Department of Psychology.

By providing an immersive, engrossing, and controlled visual and auditory experience in which participants can practice mindfulness techniques, Virtual Reality (VR) systems can create immersive, ecologically valid, first-person experiences that can even tap into physiological reactions that align with real-world experiences.

The researchers were interested in understanding if forgiveness acts as a mechanism by which mindfulness relates to relationship satisfaction. They speculated that being mindful would allow individuals to be aware of their own and their partners’ emotions in a non-judgmental and non-reactive way. The increased awareness would make people more forgiving of partner transgressions, thereby enhancing relationship satisfaction.

Emerging studies are highlighting the effectiveness of mindfulness, gratitude and hopefulness as positive psychological tools in helping people cope with anxiety and stress. These practices have also been considered beneficial in enhancing psychological health and well-being.

Dr. Khalsa is currently the Director of Clinical Operations at the Laureate Institute for Brain Research.
“…when mindfulness and self-compassion are in full bloom, they are nearly identical in a moment of suffering.”
Self-compassion actually allows us to sustain our compassion for others because we’re being compassionate to ourselves as well.

My work, over the past fifteen years has had a core theme of social support running through it, and I’d like to create an online mindfulness meditation intervention that includes a group component, such that people who have experienced cancer can meet and practice mindfulness meditation together.

I didn’t want them to needlessly struggle and suffer as much as I did, and mindfulness is one of those tools that definitely helps us all during this time. I’m helping them in the way that I wish I would have been helped.

Ultimately, my intention is for it to be a service space to help students, faculty, staff, or anyone from the community to connect with themselves. Don’t we all need to pause?

Philippe Goldin, Ph.D. is an Associate Professor at UC Davis and leads the Clinically Applied Affective Neuroscience Laboratory.

Blake Colaianne is a former Earth science teacher turned contemplative researcher. He is currently a Ph.D. Candidate in Human Development and Family Studies at Penn State University. His research focuses on supporting adolescent development using both a culture of belonging in high schools and prevention and promotion programs that teach mindfulness and compassion skills.

Michael J. Tumminia is an avid meditator, researcher, and runner. He is currently a 3rd Year Applied Developmental Psychology PhD candidate at the University of Pittsburgh.

“Whether you call it liberation, theology, transformative justice, mindfulness- we cannot separate those components of practice, all of those things are integrated. Integration brings peace, and peace within is key to embracing the other.”

Despite growing knowledge that mindfulness meditation can enhance emotional wellbeing, very little is known about how it all works. How exactly does the act of meditation help us deal with the emotional rollercoaster of everyday life? Is mindfulness training actually “transferrable” to real world situations? What’s going on in the brain? Can we even measure it?

Grant Jones (he/him) is an artist, contemplative, researcher, and activist. Currently, he is a 3rd Year Clinical Psychology PhD candidate at Harvard University and Co-Founder of The Black Lotus Collective.

How does self-compassion protect depressed adolescents? Quieting the self may be the key.

A study led by Alexandra Martelli investigated whether more mindful individuals (based on self-report measure scores) would respond to social rejection with less distress and if certain neurological mechanisms in the brain’s prefrontal cortex can potentially explain the role of mindfulness in reduced social distress.

A research team from Valencia, Spain recently investigated the effects of a brief mindfulness-based intervention on both mood and biological markers on a sample of health professional students.

A new study by Kim and colleagues explored how compassion-based training can affect two self-regulatory styles and its relationship to neural, physiological, and behavioral responses.

Dr. Ilana Nankin—the Founder & CEO of Breathe For Change—is an award-winning entrepreneur, teacher educator, and former San Francisco pre-k teacher committed to using wellness as a vehicle for healing and social change.

Torre and colleagues recruited 70 HCWs from two hospitals in Rome, Italy for a 4-week course in yoga and mindfulness.

A team of researchers based in the perceived epicenter of the virus, Wuhan, China, recently tested whether a brief mindfulness intervention delivered through an app could be effective for reducing anxiety and protecting nightly sleep during the unfolding pandemic.

Mindfulness practices can enhance a therapist’s ability to intentionally and flexibly regulate attention as well as emotional reactivity which has been demonstrated to influence burnout.

Dr. Helen Weng is a clinical psychologist and neuroscientist who originally joined the Osher Center for Integrative Medicine in 2014 as a postdoctoral scholar in the Training in Research in Integrative Medicine (TRIM) fellowship. She is developing new ways to quantify meditation skills using functional magnetic resonance imaging (fMRI) and machine learning to identify mental states of body awareness during meditation.

A new study investigated whether a brief mindfulness training designed to reduce physician burnout could be delivered through a smartphone app.

David Vago is Research Director of the Osher Center for Integrative Medicine at Vanderbilt University Medical Center.
Jeffrey Brantley, MD, is one of the founding faculty members of Duke Integrative Medicine, where he started the Mindfulness-Based Stress Reduction program in 1998.

The current study reviewed the wider scientific literature for the role of yoga and mindfulness interventions in the treatment of severe mental illness.

The amount of research involving mindfulness interventions has grown exponentially; however, only in the last decade has mindfulness research involving adolescents rapidly increased.

Mindfulness and self-compassion are theorized to disrupt the maladaptive repetition of negative thoughts and emotions for patients with chronic or mental illnesses, who are particularly susceptible to psychosocial distress.

There is promising evidence that 70% of smokers would like to quit but less than 5% of unassisted attempts at quitting are actually successful.

In a recent pilot study by Suzette Glasner, Ph.D. and her team at the Integrated Substance Abuse Programs at the David Geffen School of Medicine at UCLA, they evaluated the effects of Mindfulness-Based Relapse Prevention (MBRP) on reducing relapse susceptibility among stimulant-dependent adults receiving a contingency management (CM) intervention.

A major implication of the study suggests the distal effects of intensive retreat practice on respiration rates, a benefit not necessarily conferred by a brief, but full-day meditation session.

Researchers are exploring mindfulness-based interventions as a long-term treatment options to address the multitude of symptoms after cancer has been treated.

While the scientific study of mindfulness has exponentially increased over the past few decades, only recently has the scientific community focused on the effects of meditation training on biological aging.